The age of consent is out by seven years
It should be twenty-five.

The developmental phase of adolescence is fascinating one, and in ways unique and different to anything a person will ever experience again subsequently or previously. And a lot of that is not just about what happens to a boy’s body or a girl’s body on their way to becoming a fully grown man or woman, but is about what happens while a child’s brain starts changing into an adult brain. This period is considered a period of such tumultuous and exponential growth, that it is only just less than what occurs to a baby just after birth. And thinking back to my own adolescence, it was a period of my life beset by agony and ecstasy, fantasy and depression, mortifying embarrassment and constant painful self-consciousness. All things considered, I would not want it over again.
This period traditionally is thought to end around eighteen but that is incorrect. According to Sandra Aamodt, a neuroscientist, the science is “settled” in so far as confirming that the brain only completes its physiological development by around age twenty-five and possibly a bit earlier for females, by about two years.
This calls into question the setting of the age of consent at eighteen, since this is still seven years away from a fully formed brain and only half way through the adolescent development phase.
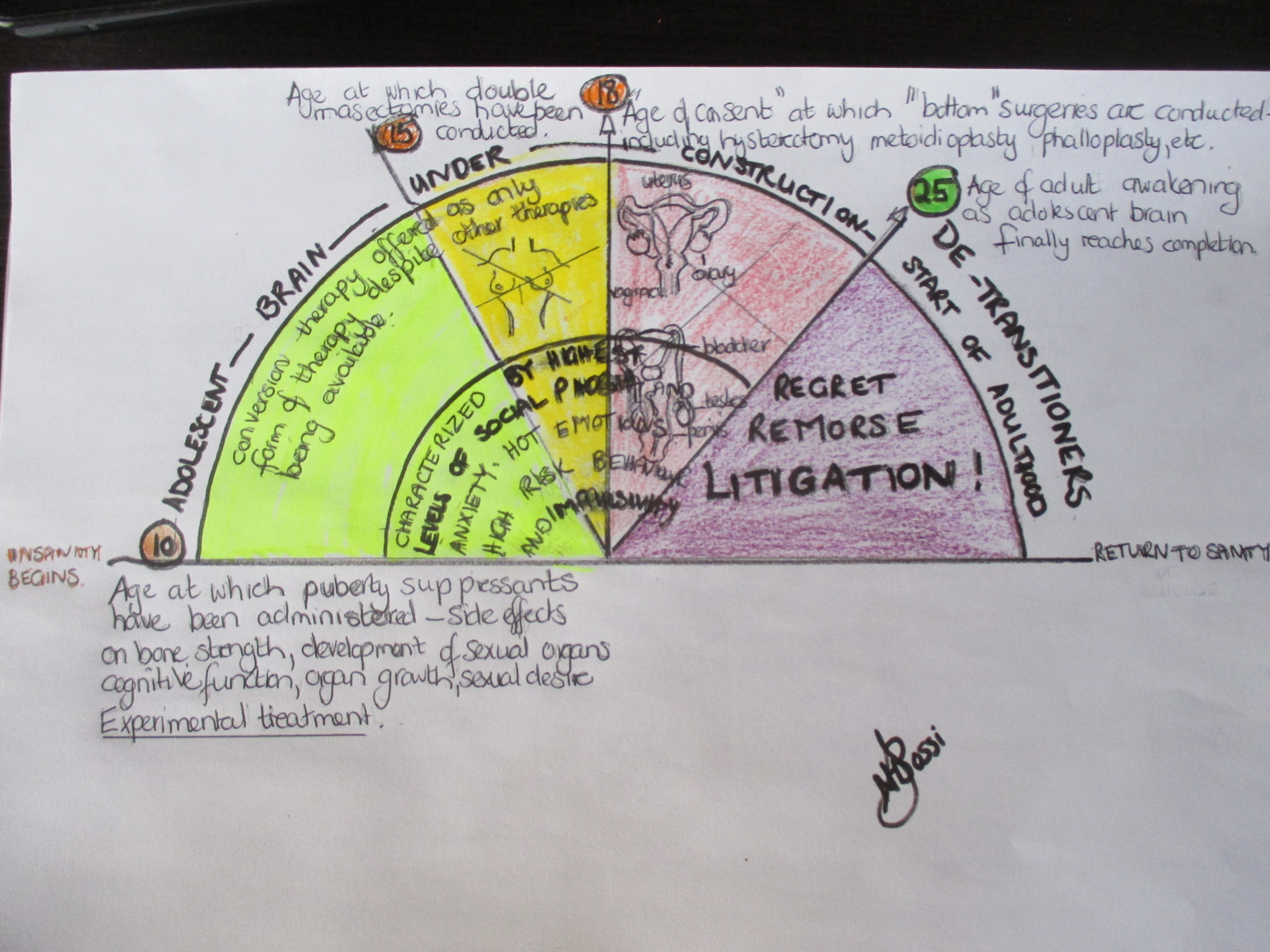
The implications of this scientifically established fact should be considered when determining whether someone is capable of making life altering decisions, which are one degree away from life threatening, and basically irreversible. Decisions such as taking puberty suppressants, gender affirming hormone therapy (GAHT) and submitting to gender affirming surgery (GAS), or in other words, sex change operations.
Sandra wrote a book called: “Welcome to the teenage brain”, which explains the neurological process that starts in puberty and ends in the mid-twenties only, firmly putting paid to the idea that an eighteen-year-old is capable of making “adult” or reasonable or far-reaching decisions. It is specifically the decision- making ability that is compromised during adolescence, because the hardware responsible for planning, goal-orientated behaviour, and thinking things though in terms of consequences, has simply not yet been fully installed. It is the process whereby concretized thinking is replaced by an ability to conceptualize, among other things.
Brain Maturity Extends Well Beyond Teen Years
In the field of addiction this information has been increasingly understood and embraced. We now understand more about why adolescents and so-called “young adults” are vulnerable to substance use and other high-risk behaviour, well into their early twenties. Because we know that their brains are not yet fully developed. This has a host of effects and implications. Why has the gender medicine sector not caught up with the science?
Another neuro-scientist, neuropsychologist Deborah Todd-Yurgelun, a PhD from Harvard University's McLean Hospital Cognitive Neuroimaging and Neuropsychology Laboratory, has together with her team, completed studies in the field of adolescent brain development and similarly established that the way the teenage brain develops, through a process akin to the sheathing of electric cables, seems to indicate a gradual process which only ends in the mid-twenties. Impulsivity and a tendency for high- risk behaviour is explained by this. An example of how this plays out in reality is described by Deborah: "Don't assume that because you've laid out the argument or presented the idea that teenagers are interpreting it in the same way you've presented it," she advises. "The frontal cortex is continuing to develop, and if you don't have the neural structure in place, the adolescent cannot really think things through at the same level as an adult." That teenage feeling
The hardware simply isn’t there for an adolescent to make decisions, so they struggle with decisions and use other parts of the brain in compensation.
Ms Todd-Yurgelun’s studies date back to 2005 and 2006. Isn’t it time to integrate this with relevant medical practices? Such as determining whether or not anyone under the age of twenty -five should be allowed to make decisions about medical interventions which: “involve significant, long-term and, in part, potentially irreversible long-term physical, and psychological consequences for young persons”.
It’s a standing joke, that insurance companies knew some of this long before science because statistics don’t lie. They found that the highest risk demographic for accidents was young males between the ages of…..eighteen and twenty-five! Why? Because without a fully formed Pre-Frontal Cortex (PFC), you are prone to taking risks, taking chances and not thinking about possible outcomes. The PFC isn’t there to say: “watch out, this could turn out badly, “or; ”remember the speed limit, you could get a fine.” I always describe the PFC as a party-pooper, putting a damper on things. But that is not all that is going on at this fraught time.
During adolescence, the reward or limbic system, (so-called primitive part of the brain) is as yet still unencumbered by the rational and reasonable PFC, and holds court. Therefore every sensation and experience is felt more intensely. It is theorized that for this reason also, adolescents’ experience of psychoactive drugs is heightened. It could explain their emotional volatility and what the neuroscientist in the Bell vs Tavistock court case calls: ”decision making” that is “hot” (i.e. more emotional), and that therefore “under 18 year-olds make less rational decisions than when the responses are made in a colder, less emotional context”. Professor Scott (Director of University College London’s Institute of Cognitive Neuroscience) was asked to testify at the court case. Based on a neuroscientific perspective, she ‘had significant doubts about the ability of young people under the age of 18 years old to adequately weigh and appreciate the significant consequences that will result from the decision to accept hormonal treatment for gender dysphoria’. She explained the neurological development of adolescents’ brains that leads to teenagers making different, more risky decisions than adults”. While Prof Scott did not question the age of 18 as being the age at which more rational decisions could be made, she did question their ability to make decisions like taking puberty blockers and hormonal therapy before this age.
It is interesting to notice that in the above quoted court case, against the Tavistock and Portman NHS Trust, the one claimant was twenty-three years old. The age at which, as a woman, neuro-imaging studies have found to be the average age for a female to fully complete the development of the pre-frontal cortex (PFC).
This claimant, Keira Bell, began taking hormone blockers in her teens, but then began the process of de-transitioning and questioned the medical practice of puberty suppression and GAHT or gender affirming hormone therapy. Please listen to her statement outside the court house: Keira Bell 'delighted' with the High Court's gender ruling against NHS Tavistock
Most of those young adults, who now deeply regret having undergone puberty blockers, sexual hormone therapy and even transitional surgery from ”top” (double mastectomy) to ”bottom” surgery (genital surgery and organ removal) are still in their twenties, having barely scraped past the age of 25, only to suddenly emerge from a “fugue” as one young woman called it. Or should we call it a fog?
Detransitioning woman left ‘heartbroken’ after irreversible surgery: ‘I was manipulated’
And never mind 18 being considered a considerable age to make institutionalized genital mutilation decisions; one young girl, was given a double mastectomy at the age of fifteen. She de-transitioned at age 16. She testified against sex change surgery and so-called treatments in front of the Senate Judiciary Committee in September 2022: My testimony against SB107 in front of Wiener and the Senate Judiciary Committee.
There she stands, questioning the adults in her world.
There are many such cases. They all speak of feeling manipulated, their parents being cajoled and bullied into believing they had no choice. Often with the threat of a teenage suicide. Yet we have had numerous studies indicating that transgenders have a higher chance of committing suicide than the general population. This process is simply not living up to expectations and, on the contrary, is causing more harm than good.
One study speaks of considerably higher risks for mortality, suicidal behaviour, and psychiatric morbidity than the general population:” Our findings suggest that sex reassignment, although alleviating gender dysphoria, may not suffice as treatment for transsexualism, and should inspire improved psychiatric and somatic care after sex reassignment for this patient group.”Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden
Other studies which have concluded similarly that the process is essentially flawed and should be abandoned completely are: Herskowitch & Dickens, 1978 and Meyer & Peter, 1979. In one study (Kockort & Farnher, 1987) more than one- half of the people who were offered sex-conversion surgery later changed their minds or became ambivalent about having the operations.”
The problem we currently have is that the whole world is gaslighting our youngsters into believing that becoming a transgender is “fun” and that it will solve all their problems. But no one can undo this Frankenstein- like procedure, once reality has hit.
Many psychologists believe it should be relegated to the psychological and medical trash heap, where procedures like lobotomies are already to be found. This is experimentation on our adolescents.
Yes, adolescents do commit suicide and increasingly so, but so-called gender affirming surgery, is NOT the solution. As we always say about suicide: this is a long- term solution to a short- term problem, and similarly, gender reassignment medications and surgeries are a long- term false promise of a solution to what is essentially a short-term problem that can be resolved in other ways. And understanding more about adolescence and the adolescent brain should have helped us realize that a long time ago. And by all accounts, we have known that it DOES NOT WORK since the 70’s. Paul Mchugh, University Distinguished Service Professor of Psychiatry at Johns Hopkins Medical School, says:” At Johns Hopkins, after pioneering sex-change surgery, we demonstrated that the practice brought no important benefits. As a result, we stopped offering that form of treatment in the 1970s.” And as to the solution: “The idea that one’s sex is a feeling, not a fact, has permeated our culture and is leaving casualties in its wake. Gender dysphoria should be treated with psychotherapy, not surgery.”
Transgenderism: A Pathogenic Meme
The ruling against Tavistock, in the Bell vs Tavistock case, was appealed and overturned, to the gleeful howl of the transgender community. But the stark facts remain; thousands of adolescents and children have been and continue to be subjected to medical butcheries, which have left them minus their sexual body parts and reproductive organs, remorseful of decisions which they were not capable of making and should not have been allowed to make, given their adolescent brains.
In the Bell vs Tavistock court case, one young de-transitioner said: “ It is only until recently that I have started to think about having children and if that is ever a possibility, I have to live with the fact that I will not be able to breastfeed my children. I still do not believe that I have fully processed the surgical procedure that I had to remove my breasts and how major it really was. I made a brash decision as a teenager, (as a lot of teenagers do) trying to find confidence and happiness, except now the rest of my life will be negatively affected. I cannot reverse any of the physical, mental or legal changes that I went through. Transition was a very temporary, superficial fix for a very complex identity issue.” Bell -v- Tavistock judgment
Here is a young adult talking about her adolescent self and admitting her own impulsivity during adolescence. We don’t let our teenagers decide if they want to leave school or have children, but we allow them to decide on whether they want to become a different sex? Who is the responsible one here? We cannot expect a teenager to take responsibility for such decisions and therefore such decisions cannot be made until the person has reached sufficient maturity.
It is heart-breaking to read this testimony and to think that adults have allowed this to happen to a vulnerable adolescent. It is a crime and should be treated as such. There is a back story to this of course and unfortunately it can be partly blamed on the Dutch for coming up with the bright idea of stepping in and interrupting the sexual development process and proposing a possibly more effective way of changing a person’s sex, as the Dutch are wont to do. But the experiment referred to as the Dutch Protocol has been found to be unsuccessful, inadequately reported on and is now being misused elsewhere as a guide to changing sex. More about this protocol can be found at: Clinical Management of Gender Dysphoria in Children and Adolescents: The Dutch Approach
De-transitioning and regret about sex change is widespread, despite the attempts by the medical industry to minimize and even dismiss them. Various websites attest to alarming and increasing numbers of young people desperately crying out for justice. They feel betrayed. The argument; that they wanted this, even demanded it, is simply ridiculous, considering what we know about adolescents and the adolescent brain. The Detransition Advocacy Network and the SexChangeRegret.com picture are Examples of such websites: The Detransition Advocacy Network, Sex Change Regret. Reading them is hair-raising and heart-breaking.
One doctor, Dr. Michael Egnor, a pediatric neurosurgeon and professor at the Renaissance School of Medicine at Stony Brook University in New York, has called this process a medical atrocity. But it continues to be endorsed by the American Medical Association, the American Academy of Pediatrics and the American Psychological Association. This endorsement runs counter to the evidence.
Fortunately, as per the Fifth Hermetic principle, the principle of Rhythm, the pendulum is starting to swing back from this insanity and voices protesting this quackery, are gaining momentum. As some speak out and voice their alarm and concern, so more medical specialists and therapists feel at liberty to speak out as well. And what about the parents? They, of course, are caught between a rock and a hard place. Anger, outrage, regret and guilt will bloody their story, but they form part of the triangle that is formed between teenager, parent and medical practitioner/therapist. And part of the problem is very much the characteristics of the teenage brain, as has been referred to here today.
Studies have also determined that adolescence is the period marked by the extreme levels of social anxiety, also referred to as social phobia; the proportions of which thankfully are never as mortifying during any other period of life, before or after. It includes an intense self-critiquing by which standards any teenager finds themselves wanting. This could explain why so many of the teenagers who transition speak of suffering social phobia and self-loathing. Many of our adolescents deal with these levels of anxiety by fleeing into a monitor and gaming, but social anxiety is intensely anxiety- provoking and debilitating. Knowing this should guide us in terms of treatment and realizing that it should abate with time. Riding it out is key and providing the adolescent with awareness about the morass that is their adolescent brain, could give them sufficient reassurance to “bytvas” as we say in Afrikaans. Hang in there, would be an adequate translation. This too shall pass. That seems to be borne out by the age at which many de-transitioners emerge from this intense “phobia”, i.e. about and around the age of twenty-five.
Other aspects of the adolescence, like the innate rebelliousness of youth, or shall we say, stubbornness, is also accounted for by this literally “immature” brain and could also explain the resistance offered by teenagers when attempts are made to talk them out of trans-gendering fantasies. “Rebellious teen behavior could stem more from biology than stubbornness”, says Yurgelun-Todd.
We as adults should have the necessary foresight and wisdom to deal with that resistance and stubbornness. And as I have stated before, these procedures should simply not be on the table at all for anyone under the age of adulthood, and that is not eighteen but closer to twenty-five.